Shaping Markets
The COMPETE Act Would Curb Anticompetitive Corporate Conduct that Harms Patients and Healthcare Workers
04. 03. 2026

The COMPETE Act (AB 1776) would, for the first time, give California a clear statutory prohibition on monopolization, monopsonization, and restraints of trade by a single dominant firm, closing a gap that currently leaves Californians with no state-level recourse when dominant hospital systems, health insurers, and pharmacy benefit managers (PBMs) use exclusionary practices, vertical integration, or buyer power to overcharge patients, squeeze healthcare workers, and crush independent pharmacies.
Unchecked market power is driving up healthcare costs while suppressing wages for nurses and healthcare workers across California
In the past, California’s healthcare system was shaped by competition among hospitals, independent pharmacies, and a range of insurers and healthcare providers vying for patients and workers. This competition helped keep healthcare costs in check, gave workers multiple employers to choose from, and sustained independent practices across the state. Today, a handful of corporate giants dominate every link of the healthcare chain, allowing them to control how much Californians pay for care and what healthcare workers earn. The top three pharmacy benefit managers (PBMs)—CVS Caremark, Express Scripts, and OptumRx—control 79% of all prescription claims in the U.S.
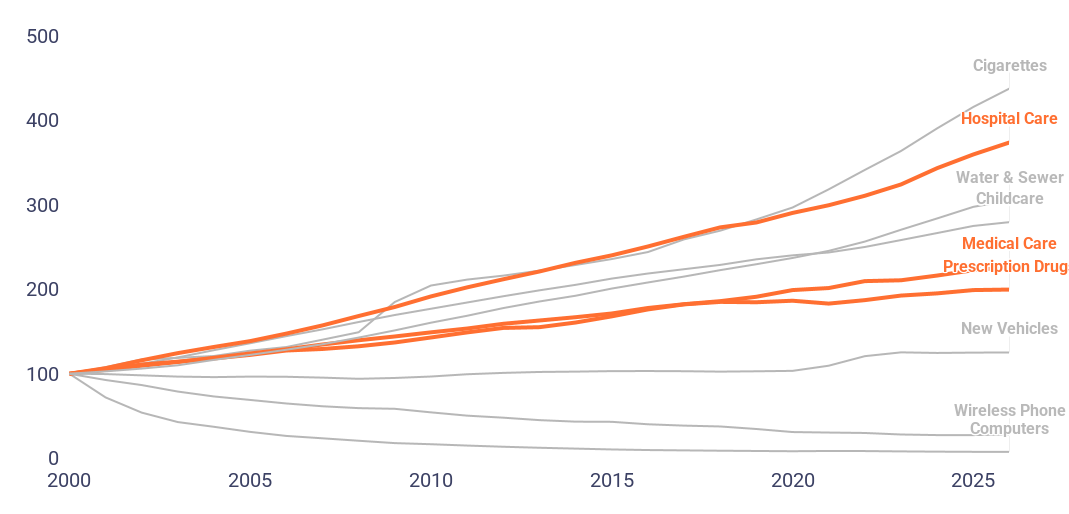
FIG. 1. U.S. HOSPITAL PRICES HAVE GROWN FASTER THAN MANY MAJOR CATEGORIES OF CONSUMPTION
Indexed BLS CPI for major categories of consumption (2000 = 100)
Without legislation to rein in unchecked anticompetitive conduct by dominant firms, troubling trends will continue:
- Patients and families will continue to pay higher healthcare costs. When a single dominant firm controls a regional healthcare market, it can raise prices without fear of being undercut. It does this by using exclusionary contracts, all-or-nothing network terms, and vertical integration to insulate itself from competition and extract higher payments from insurers, employers, and ultimately patients. Decades of hospital consolidation have left California’s hospital markets approaching monopoly levels in many counties. In California, hospitals in the largest multihospital systems have increased prices 40% more than other hospitals. Nationally, prices at monopoly hospitals are 12% higher than in markets with at least four competitors; each additional percentage point of hospital market share is associated with negotiated rates $88 to $118 higher per admission.
- Independent and community pharmacies will continue to be squeezed out by vertically integrated PBMs that play no role in developing the drugs they profit from. Independent and community pharmacies will continue to be squeezed out by vertically integrated PBMs that play no role in developing the drugs they profit from. The Big 3 PBMs, which control 79% of all U.S. prescription claims, steer prescriptions to their own affiliated pharmacies and away from independent competitors. Unlike pharmaceutical manufacturers, whose patents grant a temporary, legally-sanctioned monopoly in exchange for bringing new drugs to market, PBMs develop nothing, yet extract billions by controlling who dispenses drugs and at what price. The Big 3 PBMs’ affiliated pharmacies generated over $7.3 billion in excess revenue above acquisition costs on specialty generic drugs in just six years, marking up some lifesaving drugs by hundreds to thousands of percent—including one multiple sclerosis drug with an acquisition cost of $177 that was marked up by $3,753 per 30-day supply—while increasing their share of specialty drug dispensing revenue from 54% in 2016 to 68% in 2023.
- Nurses and healthcare workers will continue to see wages suppressed and working conditions deteriorate, even as hospital corporations report record profits. When a dominant firm controls the local market for healthcare labor, nurses have fewer employers to bargain against and wages fall. Research shows that as hospital markets have grown more concentrated, nurse wages have grown $4.08 per hour less than wages of comparable workers. Working conditions suffer too: in January 2026, 15,000 New York City nurses went on strike over unsafe staffing levels, deteriorating conditions, and threats to cut their healthcare benefits. Meanwhile, HCA Healthcare’s CEO earned approximately $24 million in 2024—a pay ratio of 391 to 1 compared to the company’s median worker.
The COMPETE Act would restore fair competition by holding single dominant firms accountable for harmful conduct by:
- Closing the single-firm loophole by making it clear that anticompetitive conduct by a monopoly is just as illegal as collusion by multiple companies.
- Holding gatekeepers accountable by prohibiting a single firm from restraining trade, such as when a dominant platform blocks competitors from reaching customers, or uses its power in one market to squeeze out rivals in another.
- Protecting workers and suppliers by explicitly covering monopsony—when a dominant buyer uses its market power to suppress wages or squeeze the businesses that sell to it. When a handful of companies control the market for buying creative work, they can drive down compensation even as their own profits grow.
- Clarifying that California courts are not bound by federal cases that are inconsistent with California’s goal of “maximally” protecting competition, including by enabling courts to take a holistic approach to curbing anticompetitive harm.